
Adult Trauma
General Approach
Amputations - Traumatic
Bites/Envenomations
Burns Thermal
Chemical Burns and Dermal Exposure
Chest Injuries/Trauma
Crush Injuries
Head Injuries
Eye Injuries
Extremity Trauma
Sexual Assault
Taser
Trauma Transportation
Trauma Alert Criteria
Tranexamic Acid (TXA)
Spinal Immobilization
General Approach to All Trauma Patients
Immediately assess all trauma patients for Trauma Alert Criteria. If criteria are met, begin transport to state approved trauma center within 10 minutes of arrival on scene whenever possible.
Basic Life Support
- Secure airway/Spinal immobilization if indicated
- Supplemental 100% oxygen if any respiratory symptoms or if pregnant > 20 weeks
-
- Including ETCO2 level (35-45 normal)
- Examine patient for obvious bleeding
- Control active bleeding with direct pressure, hemostatic gauze packing and/or tourniquet, as indicated
- Tourniquet use is now considered a Trauma Alert, regardless of red/blue criteria
- Assess Disability – neurologic status/record Glasgow coma score
- Head to toe examination to assess for injuries
- Apply physical restraints if needed to ensure patient/crew safety
- Prevent loss of body heat
- Transport pregnant patients (>20 weeks) in left lateral decubitus position, maintaining spinal immobilization as needed.
Advanced Life Support
- When condition warrants (specified as “Full ALS Assessment and Treatment” in individual protocols):
- Advanced airway/ventilatory management as needed
- Perform cardiac monitoring
- Record & monitor continuous 02 saturation and microstream capnography
- IV 0.9% NaCl KVO or IV lock
- Assess GCS score (< 8, patient should have active airway assistance- intubation, supraglottic, or BVM)
- Preferred drug for intubation is Ketamine (1 mg/kg); preferred device- Video Laryngoscope
- If BP < 90 mm Hg systolic, administer boluses of 0.9% NaCl at 250 ml until systolic BP = 90 mm Hg, unless penetrating trauma. If penetrating, no more than 1000 ml
- Administer TXA when indicated
- Assess for Tension Pneumothorax
- Tension pneumothorax should be suspected in patients who exhibit:
- Severe respiratory distress with hypoxia
- Unilateral decreased or absent lung sounds (may see tracheal deviation away from collapsed lung field)
- Evidence of hemodynamic compromise (Shock, hypotension, tachycardia, altered mental status)
- Pleural decompression for tension pneumothorax should be performed when any of the above criteria are present and likelihood of tension pneumothorax exists; decompress at 2nd intercostal space, mid-clavicular line on affected side
- In the setting of blunt traumatic cardiac arrest with suspected chest trauma, perform bilateral pleural decompressions as part of the resuscitation efforts
- Tension pneumothorax should be suspected in patients who exhibit:
- Do not delay transport to perform procedures on scene unless immediately needed to stabilize patient (e.g. airway management, hemorrhage control)
Contact Medical Control for Additional Orders if Needed
Amputations - Traumatic
Basic Life Support
- If amputation incomplete:
- Attempt to stabilize with bulky pressure dressing
- Splint inline
- If amputation complete:
- Cleanse amputated part with sterile saline
- Wrap in sterile dressing soaked in sterile saline
- Place in plastic bag if possible
- Attempt to cool with cool pack (outside the plastic bag) during transport
Advanced Life Support
- For isolated extremity trauma:
- Fentanyl (Sublimaze) 1 mcg/kg (maximum 100 mcg) slow IV; repeat once after 5 minutes as needed OR 100 mcg intranasal via MAD (divide dose equally between each nare). Maximum cumulative dose is 200 mcg
- Hold if Systolic Bp <100
- Fentanyl (Sublimaze) 1 mcg/kg (maximum 100 mcg) slow IV; repeat once after 5 minutes as needed OR 100 mcg intranasal via MAD (divide dose equally between each nare). Maximum cumulative dose is 200 mcg
- For uncontrollable hemorrhage:
-
- Apply tourniquet device 4-6 inches proximal to bleeding site
- Tourniquet must be at least 1 ½ inches wide or an approved commercially available product
- Do not apply over joint
- Tighten tourniquet until bright red bleeding has stopped
- Document time of placement on the tourniquet or the patient
- Secure in place and expedite transport to SATC (State Approved Trauma Center)
- Notify receiving center of presence and location of tourniquet
- Administer TXA when indicated
Bites and Envenomations
Basic Life Support
- Irrigate/Cleanse wound with 0.9% NaCl (remove any large debris)
- Remove stinger if wasp or bee (if easily removed)
- Mark initial edematous area with pen and note time
- Immobilize affected part
- If extremity bite/sting, remove jewelry of affected extremity
- Attempt to identify what caused bite (take picture and bring the picture to ER if possible)
Advanced Life Support
- For hypotension (systolic BP < 90 mmHg) not improved by fluid boluses, or when fluid boluses are contraindicated
- Norepinephrine infusion at 0.5-16 mcg/minute IV/IO, titrated to maintain SBP > 90 mm Hg (see infusion preparation chart) OR
- Push dose epinephrine: Remove 9ml (0.9mg) of 1:10,000 Epinephrine from the pre-filled syringe then draw 9ml of NS into the pre-filled syringe and mix solution. Concentration 10mcg/ml. IV push 1ml every minute to increase blood pressure to 90 mmHg; max 10ml (100mcg).
- For Black Widow spider or Scorpion envenomation with severe muscle spasms
- Midazolam (Versed) 5 mg IM or intranasal via MAD OR 2.5 mg slow IV
- For patients with severe pain if systolic blood pressure >100 mmHg:
- Fentanyl (Sublimaze) 1 mcg/kg (maximum 100 mcg) slow IV; repeat once after 5 minutes as needed OR 100 mcg intranasal via MAD (divide dose equally between each nare). Maximum cumulative dose is 200 mcg
- Preferentially use intranasal delivery via MAD for those where IV access may be difficult to obtain in a timely fashion or not indicated for chief complaint
- Fentanyl (Sublimaze) 1 mcg/kg (maximum 100 mcg) slow IV; repeat once after 5 minutes as needed OR 100 mcg intranasal via MAD (divide dose equally between each nare). Maximum cumulative dose is 200 mcg
- Transport Snake envenomations to nearest State Approved Trauma Center
Contact Medical Control for Additional Orders if Needed
Burns - Thermal
Basic Life Support
- Remove clothing; cool heat source if tar or asphalt; otherwise prevent hypothermia
- Cool dressings on minor (small area) burns with sterile saline (do not use ice packs)
- Dry, clean burn sheet on:
- 2° burns greater than 10% of Body Surface Area
- 3° burns
- Electrical and chemical burns (after decontamination if indicated)
- Spinal immobilization if high voltage electrical injuries (>1000 Volts, excluding Taser) or lightning injury
- Prevent Hypothermia; only wash burns that require decontamination (gasoline or hazmat substance)
- Consider spinal immobilization if other trauma is suspected or unknown
Advanced Life Support
- Pain management is very important! If moderate or severe pain:
- Fentanyl (Sublimaze) 1 mcg/kg (maximum 100 mcg) slow IV; repeat once after 5 minutes as needed OR 100 mcg intranasal via MAD (divide dose equally between each nare). Maximum cumulative dose is 200 mcg
- Preferentially use intranasal delivery via MAD for those where IV access may be difficult to obtain in a timely fashion
- Hold if systolic <100
- Preferentially use intranasal delivery via MAD for those where IV access may be difficult to obtain in a timely fashion
- Fentanyl (Sublimaze) 1 mcg/kg (maximum 100 mcg) slow IV; repeat once after 5 minutes as needed OR 100 mcg intranasal via MAD (divide dose equally between each nare). Maximum cumulative dose is 200 mcg
- Use with caution in inhalation injuries
- Administer IV 0.9% NaCl per the following American Burn Association Guidelines IF BURNS > 20% BSA
- 0-5 years old 125 ml/hr
- 6-13 years old 250 ml/hr
- > 14 years old 500 ml/hr
- If the patient meets any of the below criteria, transport to the nearest Burn Center
- Burns ≥ 10% TBSA
- Burns to face, hands, feet, genitalia, perineum, or major joints
- 3rd degree burns to any age group
- Electrical burns, including lightning injury
- Chemical burns
- Inhalation injury
- Burn injury in patients with preexisting medical disorders that could complicate management, prolong recovery, or affect mortality
- Any patients with burns and other traumatic injuries in which the burn injury poses the greatest risk of morbidity or mortality. In such cases, if the trauma poses the greater immediate risk, the patient may be transported to the trauma center for stabilization and then transferred to the burn center.
Contact Medical Control for Additional Orders if Needed
Chemical Burns and Dermal Exposure
Basic Life Support
- Stop the burning process
- Remove all clothing prior to irrigation
- If a caustic liquid is involved, flush with copious amounts of water
- If a dry chemical is involved, brush it off, then flush with copious amounts of water
- Do not use water for elemental metals (sodium, potassium, lithium) and phenol: Remove obvious metallic fragments from skin and cover the burn with mineral oil or cooking oil. As a last resort use extremely large amounts of soap and water with continuous irrigation until all phenols are removed
- For chemical burns with eye involvement, immediately begin flushing the eye with normal saline and continue throughout assessment and transport
- Apply a burn sheet or dry clean dressing to burn areas
- Transport to Burn Center
Advanced Life Support
- For inhaled toxin with acute bronchospasm:
- Albuterol (Proventil) 2.5 mg/3 ml and Ipratropium Bromide 0.02% (Atrovent) 0.5mg/2.5 ml via nebulizer
- Repeat Albuterol (Proventil)/Ipratropium Bromide (Atrovent) X 2 if wheezing persists
- For persistent burning sensation of the airways (after Albuterol/Atrovent) administer Sodium Bicarbonate (4.2%) 5 ml via nebulizer
- Observe for signs of impending respiratory failure
Contact Medical Control for Additional Orders if Needed
Chest Injuries/Trauma
Basic Life Support
- Assess breath sounds frequently
- Assess for ventilatory compromise and assist with BVM as needed
- For Open/Sucking Chest wounds, apply occlusive dressing sealed on three sides or commercially approved device
- Remove temporarily to vent air if respiratory status worsens
Advanced Life Support
- Full ALS Assessment and Treatment
- Total amount of IVF should not exceed 1000 ml in penetrating trauma
- Assess for flail segment and tension pneumothorax
- Observe for signs of impending respiratory failure; Refer to the Airway Management Protocol if needed:
- Hypoxia (O2 Sat <90) not improved by 100% Oxygen
- Poor ventilatory effort, monitor ETCO2 continuous waveform
- Altered mental status/ decreased level of consciousness
- Inability to maintain patent airway
- If age 55 or older, transport to nearest SATC
- Administer TXA when indicated
Contact Medical Control for Additional Orders if Needed
Crush Injuries
Crush Injury should be suspected in patients who have a large area of their body subjected to a heavy force for a prolonged period of time. Upon release, patients may become hypovolemic and hyperkalemic. Hyperkalemia can lead to lethal arrhythmias.
Basic Life Support
- Secure airway/Spinal immobilization if indicated
- Supplemental 100% oxygen if any respiratory symptoms
- Including ETCO2 level (35-45 normal)
- Examine patient for obvious bleeding
- Control active bleeding with direct pressure, hemostatic gauze packing and/or tourniquet, as indicated
- Assess Disability – neurologic status/record Glasgow coma score
- Head to toe examination to assess for injuries
- Apply physical restraints if needed to ensure patient/crew safety
- Prevent loss of body heat
Advanced Life Support
- Advanced airway/ventilatory management as needed
- Perform cardiac monitoring
- Record & monitor continuous 02 saturation and microstream capnography
- Fentanyl (Sublimaze) 1 mcg/kg (maximum 100 mcg) slow IV; repeat once after 5 minutes as needed OR 100 mcg intranasal via MAD (divide dose equally between each nare). Maximum cumulative dose is 200 mcg
- Hold if systolic <100
- Obtain 2 large bore IV’s. Administer IV 0.9% NaCl prior to extrication to maintain systolic >90
- Administer 1mEq/kg IV/IO of Sodium Bicarbonate (max 50mEq)
- IO if unable to obtain IV
- Perform diagnostic 12 lead
- Administer TXA when indicated
- Treat signs of hyperkalemia: EKG with Peaked T waves, absent p waves, or widened QRS
- Albuterol (Proventil) 2.5 mg/3 ml
- Sodium bicarbonate 1 mEq/kg IV/IO (max 50mEq)
- Calcium chloride 1 gram IV/IO
Contact Medical Control for Additional Orders if Needed
Head injuries
Airway interventions can be detrimental in patients with head injury by raising intracranial pressure, worsening hypoxia (and secondary brain injury) and increasing risk of aspiration.
Whenever possible, these patients should be managed in the least invasive manner to maintain O2 saturation > 90% (i.e. NRBM, BVM or supraglottic device with 100% O2). Patients with GCS <8 should have active airway management (BVM, supraglottic device, intubation). Placement of a non-rebreather is not considered active airway management.
Basic Life Support
- Supplemental oxygen
- Restrain as needed
- If Normotensive or Hypertensive elevate head of backboard 15°-30° (reverse Trendelenburg)
Advanced Life Support
- Full ALS Assessment and Treatment
- Advanced airway/ventilatory management as needed
- Observe for signs of impending respiratory failure; Refer to the Airway Management Protocol if needed. Any of the following criteria require active airway assistance (BVM, supraglottic,intubation)
- Hypoxia (O2 Sat <90) not improved by 100% Oxygen
- Poor ventilatory effort (increasing ETCO2)
- Altered mental status/ decreased level of consciousness (GCS 8 or less)
- Inability to maintain patent airway
- Observe for signs of impending respiratory failure; Refer to the Airway Management Protocol if needed. Any of the following criteria require active airway assistance (BVM, supraglottic,intubation)
- For patients with assisted ventilation administer eucapneic (normal rate 12-15/minute) ventilations with a goal of ETCO2 between 35-40 mmHg
- Acute herniation should be suspected when the following signs are present:
- Acute unilateral dilated and nonreactive pupil
- Abrupt deterioration in mental status
- Abrupt onset of motor posturing
- Hyperventilation (ventilatory rate of 20) is a temporizing measure which is only indicated in the event of acute herniation
- If signs of acute herniation develop, increase ventilatory rate to 20/minute with a goal of ETCO2 between 30-35 mmHg
- Hyperventilation (ventilatory rate of 20) is a temporizing measure which is only indicated in the event of acute herniation
- Acute herniation should be suspected when the following signs are present:
- Avoid hypotension (SBP <100)
- Administer fluid bolus as needed per protocol
- Push dose epinephrine: Remove 9ml (0.9mg) of 1:10,000 Epinephrine from the pre-filled syringe then draw 9ml of NS into the pre-filled syringe and mix solution. Concentration 10mcg/ml. IV push 1ml every minute to increase blood pressure to 90 mmHg; max 10ml (100mcg).
- For awake patients experiencing nausea or vomiting administer Ondansetron (Zofran), 4 mg slow IV or 4 mg Oral Disintegrating Tablet (ODT) by mouth may repeat every 5 mins, max 8 mg
- Apply physical restraints if needed to ensure patient/crew safety
- If patient is combative to the point of injuring his/herself or the crew
- Preferred: Ketamine 1mg/kg IM (max 100mg) or 0.5mg/kg IV/IO (max 50mg)
- Contact Medical Control for Additional Orders if Needed
Eye Injuries
Basic Life Support
- Stabilize any penetrating objects
- Do not remove any impaled object
- Protective metal shield unless impaled object precludes
- Prevent patient from bending or straining
- If blood observed in anterior chamber, transport with head elevated 60°
Contact Medical Control for Additional Orders if Needed
Extremity Trauma
Basic Life Support
- Remove or cut away clothing to expose area of injury
- Control active bleeding with direct pressure, hemostatic gauze packing and/or tourniquet, as indicated
- Check distal pulses, capillary refill, sensation/movement prior to splinting
- If pulse present, splint in position found if possible
- If pulse absent, attempt to place the injury into anatomical position and reassess pulses
- Open wounds/fractures should be covered with sterile dressings and immobilized in the presenting position
- Dislocations should be immobilized to prevent any further movement of the joint
- Check distal pulses, capillary refill, and sensation after splinting
Advanced Life Support
- For isolated extremity trauma:
- Fentanyl (Sublimaze) 1 mcg/kg (maximum 100 mcg) slow IV; repeat once after 5 minutes as needed OR 100 mcg intranasal via MAD (divide dose equally between each nare). Maximum cumulative dose is 200 mcg
- Consider pain control only after SBP >100
- For uncontrollable hemorrhage:
- Apply tourniquet device 4-6 inches proximal to bleeding site
- Tourniquet must be at least 1 1/2 inches wide
- Do not apply over a joint
- Tighten tourniquet until bright red bleeding has stopped
- Document time of placement on the tourniquet or the patient
- Secure in place and expedite transport to SATC (State Approved Trauma Center)
- Meet trauma alert criteria
- Notify receiving center of presence and location of tourniquet
- Apply tourniquet device 4-6 inches proximal to bleeding site
- If the wound is located in an area where use of tourniquet is not feasible (groin, axilla), aggressively pack the wound with hemostatic gauze until the bleeding stops
- For limbs that remain entrapped despite all other extrication attempts contact Medical Control to arrange for on-scene medical direction.
Contact Medical Control for Additional Orders if Needed
Sexual Assault
- For victims of sexual assault who meet Trauma Alert criteria, transport to State Approved Trauma Center.
- For all other cases, transport to the closest appropriate facility
- Provide supportive care as indicated by patient’s condition
- Preserve any evidence (clothing, personal belongings) and transport with the patient
Taser
For patients who have been controlled by law enforcement using a Taser device; also refer to any protocol that applies to underlying conditions (e.g. behavioral emergencies, cocaine/ sympathomimetic toxicity, etc). Voltage alone does not require patient to be trauma alerted.
Basic Life Support
- Confirm scene safety with law enforcement
- Turn patient supine if found in a prone position
- Secure the Taser prongs in place if not removed by law enforcement
- Do not remove the prongs if lodged in the patient and left in place by law enforcement unless there is interference with important patient care measures
Advanced Life Support
- If the patient requires Chemical or Physical restraints perform Full ALS Assessment and Treatment (this includes continuous vital sign monitoring)
- For patients with severe agitation resulting in interference with patient care or patient/ crew safety, or for patients who continue to struggle against physical restraints refer to the Behavioral Emergencies protocol
- Transport patient supine or lateral recumbent position only
- Patient transport in the prone position is contraindicated
Note: All patients transported after a taser event, shall have a 12
Contact Medical Control for Additional Orders if Needed
Trauma Transportation
Hospital Destination for Trauma Patients
The following patients are required to be transported to a State Approved Trauma Center:
- Patients who meet the Trauma Alert criteria as specified in the Osceola County EMS protocols
- Patients who meet the Trauma Gray criteria as specified in the Osceola County EMS protocols
To avoid a delay in definitive management, strongly consider transport to a trauma center if any of these are present:
- MCC rider separated from vehicle with significant impact
- Pedestrian/Bicyclist thrown, crushed, run over, or with significant impact
- Concerns for intoxication/impairment in the setting of trauma
Dispatch Procedures - Ground:
- In Osceola County, there are three ground advance life support emergency medical service providers: Kissimmee Fire Department (KFD), Osceola County Fire and Emergency Service (OCFES), St. Cloud Fire Rescue (SCFR). Requests for emergency services are dispatched through an enhanced 9-1-1 system. The enhancements allow the location and telephone number of the caller to be instantaneously displayed on the 9-1-1 call taker's computer screen at one of three primary Public Safety Answering Points (PSAPs). The caller's location (or cell site for cellular calls) determines which emergency answering point receives that particular request for emergency assistance. If the normally designated PSAP for that locale is busy, the call is automatically routed to an alternate answering point. Staffing for the primary PSAPs is provided by Kissimmee Police Department, Osceola County Sherriff’s Office and St. Cloud Police Department.
- The Primary PSAPs and their area of responsibility are:
- Kissimmee Police Department (KPD): all of the City of Kissimmee
- Osceola County Sherriff’s Department: all of unincorporated Osceola County
- St. Cloud Police Department: all of the City of St. Cloud
- The Primary PSAPs and their area of responsibility are:
- The 9-1-1 call taker relies on the address information provided by the caller as primary dispatch information, using the screen display only as secondary or backup information. The public safety call taker may also require a call back number. Generally, wireless phone calls provide the 9-1-1 system with the caller’s phone number and longitude, latitude coordinates, but the call taker still obtains location and call back numbers from all cellular callers.
- Each PSAP is equipped with telecommunications devices for the deaf (TDDs). Every PSAP can also refer callers to AT&T's language line if in-house interpreters are not available.
- Osceola County, Kissimmee and St. Cloud PSAPs have received specialized training in emergency medical dispatch.
- Unincorporated Osceola County, Kissimmee and St. Cloud: Requests for emergency medical assistance originating in these jurisdictions are dispatched within their respective PSAPs.
- Florida State Road Emergencies: Florida Highway Patrol (FHP) is a primary PSAP for *FHP cellular phone calls only. All PSAPs within the County can refer calls in their jurisdiction that jointly falls on FHP's territory.
- If a call is received requesting emergency medical assistance at any of PSAPs and it is determined the incident did not originate within their jurisdiction, the call can be transferred to the appropriate PSAP by pressing one button.
- General public requests for emergency medical assistance
- The emergency medical dispatcher is responsible for providing prearrival medical instructions where appropriate, and obtaining the following information when answering all incoming phone lines, regardless of origin:
- Numerical address or intersection where ALS assistance is needed.
- Number of patients
- Other specific information according to emergency medical dispatch (EMD) protocols to include the extent and severity of reported injuries
- Verify address where assistance is needed
- Verify nearest cross street to address, particularly when address is showing nonunique status
- Verify call-back phone number (Obtain cellular call-back phone number wherever applicable)
- Scene hazards
- The emergency medical dispatcher is responsible for providing prearrival medical instructions where appropriate, and obtaining the following information when answering all incoming phone lines, regardless of origin:
- In Osceola County, all emergency medical dispatch PSAPs have adopted the nationally recognized Medical Priority Dispatch System into their standard operating procedure to decide the appropriate level of response (personnel, equipment and vehicles) to send to a scene. While emergency medical dispatch caller interrogation algorithms are uniform across agencies, deployment practices necessarily vary because of differences in population distribution and emergency medical resources in the Osceola County trauma system.
- Kissimmee, St. Cloud and Osceola County operate separate emergency medical services response systems. The emergency medical dispatcher of each will be responsible for:
- Dispatching all calls within his respective jurisdiction in priority sequence.
- Promptly acknowledging all radio transmissions, and maintaining appropriate response coverage.
- Tracking current unit status to ensure proper unit selection by the Computer Aided Dispatch (CAD) system. The closest available unit should be responded to a call for assistance. The CAD system will be the initial source of information for determining that closest unit. An available unit not in station may be considered for deployment. Examples of such circumstances can include:
- A unit "on the air" closest to the call will be responded over a unit that is in its station.
- The emergency medical dispatcher will refer to the jurisdiction's dispatch procedure for zoning, if appropriate.
- Additional emergency response agencies will be used when necessary. All dispatch centers have access to emergency resources through radio communications if available, or by telephone if necessary, to request assistance. On-scene personnel must identify the emergency resources needed (i.e. additional ALS units, Fire Apparatus, Utilities, Law Enforcement)
- For the efficient day-to-day operation of the Osceola County trauma system, formal and informal mutual aid agreements exist among the emergency medical transport services within Osceola County and between specific outlying counties to supplement equipment and personnel on an ad hoc basis. Depending on the severity and extent of an incident, a graduated approach for additional assistance is followed when local emergency medical response needs exceed the capacity of the requested ALS ground emergency medical transport service.
Dispatch Procedures - Air:
- There are five air ambulance services available to Osceola County: Air Care, Aeromed, First Flight, Bay Flight and St. Lucie County Sheriffs Air Rescue 1. Any recognized public safety responder on-scene can request a standby or launch of a helicopter to transport a potential trauma alert. This type of scene request may be relayed through the emergency medical dispatcher through that agency's own dispatch center to the air medical communication specialist.
- The assignment of the air medical agency is made by the emergency medical dispatcher according to the closest air medical service to the incident scene.
- If the closest service is not available the next closest service will be called
- The emergency medical dispatcher will be as specific as possible when contacting the air medical communication specialist by providing the following information:
- Location of incident to include numerical address cross-streets and if possible, GPS coordinates
- Radio frequency, contact unit name and ID# of the landing zone (LZ) commander
Adult & Pediatric Trauma Alert Procedure:
- Assess the trauma patient and determine the need for transportation to the State Approved Trauma Center (SATC) using the adult or pediatric trauma criteria:
- A "Trauma Alert" is to be initiated immediately when an adult or pediatric trauma patient is determined to meet the adult or pediatric trauma alert criteria
- Patients meeting Trauma Alert criteria will be transported to the nearest available SATC
- All Trauma Alert patients 15 years of age or less will be transported to the State Approved Pediatric Trauma Center (SAPTC).
- Once a Trauma Alert has been initiated, contact the receiving facility and provide initial notification that a Trauma Alert patient will be transported, or is en route:
- Give agency name and unit number, paramedic/EMT number, incident location, brief description of injury and estimated time of arrival
- Be specific as to the actual Trauma Alert criteria when possible
- Use the term "Trauma Alert" to avoid any confusion
- Give agency name and unit number, paramedic/EMT number, incident location, brief description of injury and estimated time of arrival
- When en route, the transporting crew will re-contact the SATC and provide a radio report, as outlined in the Radio Report Format section
- The transporting agency will provide a completed Patient Care Report to the hospital staff upon delivery of patient to the SATC, or other appropriate facility
- All medical care will be provided in accordance with condition specific protocols or Medical Control orders
- Trauma Alert patients may also be transported to the nearest emergency department (other than a State Approved Trauma Center) when the following conditions exist:
- Cardiac arrest on initial patient assessment following trauma
- Unmanageable airway emergencies
- Logistical failures that make transport to SATC impossible
Transport Mode
- The route (air or ground) that enables the patient to arrive at the trauma center in the shortest time shall be used
- Traumatic cardiac arrest is a contraindication to initiating helicopter transport
- An exception to this principle is when the arrest occurs during the transition of the patient to the helicopter (this may include transport in a ground unit to the landing zone)
|
Central Florida State Approved Trauma Centers |
||
|
Orlando Regional Medical Center* |
Level I |
Orlando |
|
Arnold Palmer Children’s Hospital |
Level 1 Pediatric |
Orlando |
|
Tampa General Hospital* |
Level I |
Tampa |
|
Osceola Regional Medical Center |
Level II |
Kissimmee |
|
Lakeland Regional Medical Center |
Level II |
Lakeland |
|
Holmes Regional Medical Center |
Level II |
Melbourne |
|
Lawnwood Regional Medical Center |
Level II |
Fort Pierce |
*Recognized Regional Burn Center
Emergency Interfacility Transfer of Trauma Victims
Patients may occasionally require emergency interfacility transfer from an outlying hospital to a State Approved Trauma Center (SATC). The decision to initiate this level of interfacility transfer is made by the treating physician at the outlying hospital, in coordination with the accepting physician at the SATC.
When this scenario arises, adhere to the following:
- Notify Medical Control as soon as possible on any request for Interfacility Transport
- Assess the patient upon arrival, but avoid unnecessary delays in transport
- Transport to the facility at which a physician has accepted the patient unless
- Operationally unfeasible
- There is no accepting physician
- During transport, the patient experiences unforeseen life-threatening events requiring immediate intervention (i.e. cardiac arrest, unstable airway)
*in which case, the patient will be transported to the nearest most appropriate hospital
If EMS crew members have not received training on, and /or are not capable of managing devices or medications that must be continued during transport, an adequately trained care provider from the transferring facility must accompany the patient during transport
- If the hospital is refusing to send someone, contact medical control
Contact Medical Control for Additional Orders if Needed
Adult Trauma Alert Criteria
The presence of any of the 4 listed items below requires Trauma Alert Activation
- Meets color coded triage system (any one RED, or any two BLUE criteria met) Gray criteria should be transported to the nearest SATC but do not require an alert, unless red and/or blue criteria met.
- GCS ≤ 12 (GCS is a stand-alone criteria, even if color coded criteria not met)
- Meets Local Criteria: High Voltage Electrical Injury (>1000 volts), hanging, drowning if diving injury suspected, tourniquet in place and bites/envenomations (snake)
- Does not meet above criteria but paramedic judgment indicates patient may need trauma capable facility
|
Component |
BLUE Criteria |
RED Criteria |
Gray Criteria | |
|
Airway |
Respiratory rate ≥ 30 |
Active airway assistance1 |
||
|
Circulation |
Sustained heart rate ≥ 120 |
Any of the following:
|
||
|
Best Motor Response (Glasgow Coma Scale) |
BMR of 5 |
Any of the following:
|
||
|
Cutaneous |
Any of the following:
|
Any of the following:
|
Any patients with external manifestation of blunt head, chest or abdominal trauma who meet the following criteria: | |
|
Long Bone Fracture4 |
Any of the following:
|
Fracture of 2 or more long bones4 |
||
|
Age |
55 year or older |
N/A |
|
|
|
Mechanism of Injury |
Any of the following:
|
|
|
BLUE = any two (2) – transport as a trauma alert
RED = any one (1) – transport as a trauma alert
- Airway assistance beyond administration of oxygen
- Major degloving injuries, or major flap avulsion (>5 in.)
- Excluding superficial wounds in which the depth of the wound can be determined
- Longbones include humerus, radius + ulna, femur, tibia + fibula
- Excluding moped, all terrain vehicle, bicycle, or open body of a pickup truck or open top vehicle
- Only applies to driver of vehicle
- If the trauma poses the greater immediate risk, the patient may be transported to the trauma center for stabilization and then transferred to the burn center. Otherwise, patient should be transported to the nearest Burn Center
IF GROUND TRANSPORT OF A TRAUMA ALERT IS ESTIMATED TO TAKE LONGER THAN 20 MINUTES AIR TRANSPORT SHOULD BE CONSIDERED.
Trauma Gray Criteria
- Immediately assess all trauma patients for Trauma Alert Criteria. If trauma alert or Trauma Gray criteria are met, begin transport to SATC within 10 minutes of arrival on scene whenever possible.
- All Patients meeting the following criteria, who do not meet Trauma Alert criteria will automatically be classified as a “Trauma Gray” and should be transported to the nearest Trauma center.
- Any patients with external manifestation of blunt head, chest or abdominal trauma who meet the following criteria:
- Age 65 or older OR
- History of cirrhosis or bleeding disorder OR
- On systemic anticoagulation or antiplatlet agents. Examples may include:
- Apixiban (Eliquis)
- Betrixaban (Bevyxxa)
- Dabigatran (Pradaxa)
- Edoxabam (Savaysa)
- Enoxaparin (Lovenox)
- Rivaroxiban (Xarelto)
- Warfarin (Coumadin)
- Clopidrogel (Plavix)
- Ticagrelor (Brilinta)
- Prasugrel (Effient)
- Cangrelor (Kangreal)
- Vopraxar (Zontivity)
Contact Medical Control for Additional Orders if Needed
Tranexamic Acid (TXA) - Indications
Suspected life-threatening hemorrhage in the setting of trauma (without an isolated head injury and within 3 hours of injury).
- Systolic <90mmHg, MAP <65, or sustained HR> 110
- Adult: Administer 1g in 100ml NS over 10 minutes IV/IO
- Pediatric: 15mg/kg (1g max) in 100ml NS over 10 minutes IV/IO
- Trauma Arrest if loss of pulses after patient contact with PEA
- Do not delay transport to perform procedures on scene unless immediately needed to stabilize patient (airway management, hemorrhage control)
- Ensure that the receiving SATC is aware that TXA was administered
Pelvic Binder Use
A pelvic binder provides early stabilization for the hemodynamically unstable patient who has a suspected or confirmed unstable pelvic fracture. It reduces the pelvic volume and reduces movement, which tamponades bleeding and reduces the risk of shearing major blood vessels during transport. A pelvic binder should be applied to patients who meet the following criteria:
Indications:
- Hemodynamic instability AND a suspected or confirmed pelvic fracture
OR
- An unstable pelvic fracture diagnosed on physical exam
OR
- Mechanism of injury consistent with possible fracture with hemorrhagic shock without another source of hemorrhage
Spinal Immobilization - Indications
Determining the need for spinal immobilization requires a careful assessment of the patient's:
- Mechanism of injury
- Mental status and ability to recognize the presence of spinal injury symptoms
- Physical complaints and overall condition
The following algorithms (Blunt and Penetrating Trauma) can be used to assist paramedics in making the most appropriate decision about the need for spinal Immobilization. Cervical spine immobilization and long board immobilization are separate entities and should be treated as such. If a patient has neck pain only, cervical collar should be applied with the following guidelines.
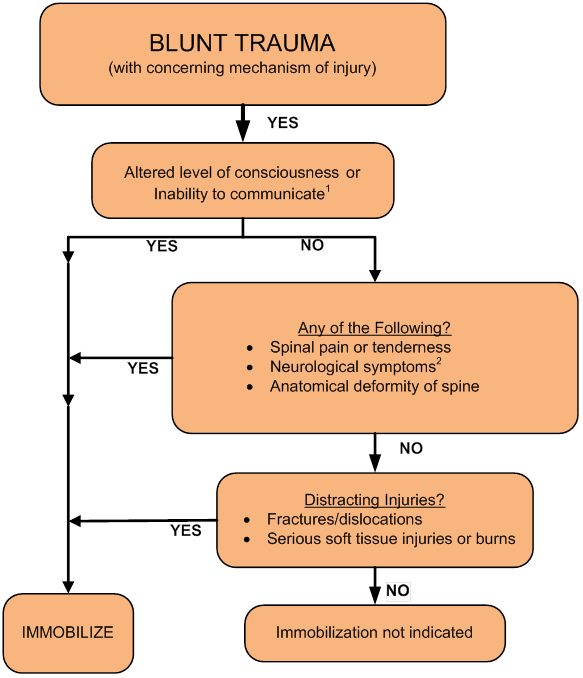
Blunt Trauma with Concerning Mechanism of Injury
Concerning mechanism of injury defined as:
- Any mechanism that produces a violent impact on the head, neck, torso or pelvis
- Incidents that produce sudden acceleration or deceleration, including lateral bending forces
- Any fall, especially in the elderly
- Ejection or fall from a moving mode of transportation
Immobilize if any of the following exist:
- Altered level of consciousness or inability to communicate:
- Abnormal GCS
- Evidence of significant intoxication
- Dementia
- Speech or hearing impairment
- Age (young children)
- Language barrier
- Complaints suggestive of spinal injury:
- Spinal pain or tenderness, including paraspinal musculature
- Neurologic deficit or complaint, including parasthesia, paralysis or weakness
- Anatomical deformity of the spine
- Distracting Injuries:
- Long bone fractures
- Joint dislocations
- Abdominal or thoracic pain, or obvious visceral injury
- Large lacerations, degloving injuries or crush injuries
- Serious burns
- Any injury producing acute functional impairment
* IF IN DOUBT, IMMOBILIZE *
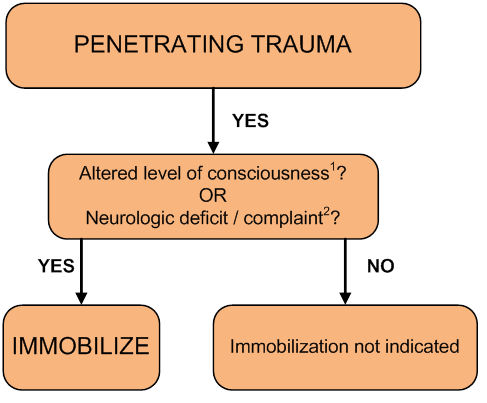
Penetrating Trauma
Immobilize if any of the following exist:
- Altered level of consciousness
- Any neurological deficits1 or complaints
- Test motor function in both upper and lower extremities (entire extremity)
- Test sensation in both upper and lower extremities (start proximal and work towards hands and feet)
- Ask about numbness or tingling in extremities
- Examples are numbness, focal weakness, focal sensory deficit, parasthesias. Identifying the presence of neurological signs and symptoms requires careful assessment and history taking.
* IF IN DOUBT, IMMOBILIZE *
Other Situations
- Spinal precautions can be maintained by application of a cervical collar and securing patient firmly to the stretcher without a long backboard if all 5 of these criteria are met:
- Patient is ambulatory at the scene
- Patient does not demonstrate an altered level of consciousness or inability to communicate
- Patient does not have complaints suggestive of spinal injury
- Patient does not have distracting injuries
- Immobilize all patients with the following conditions:
- High voltage electrical injuries (does not include Taser use), lightning injuries
- Shallow water drowning and/or diving injuries
- If spinal immobilization is indicated but refused by the patient:
- Advise the patient of the indication for immobilization, and the risks of refusing the intervention
- If the patient allows, apply the cervical collar even if backboard is refused
- Maintain spinal alignment as best as can be achieved during transport
- CLEARLY DOCUMENT REFUSAL OF IMMOBILIZATION
- If spinal immobilization is indicated but the patient cannot tolerate supine position:
- Apply all elements of spinal immobilization that the patient will tolerate
- Maintain spinal alignment as best as can be achieved during transport, if patient is found in a position which inhibits immobilization, maintain this alignment and transport.
- CLEARLY DOCUMENT THE CLINICAL CONDITION THAT INTERFERED WITH FULL IMMOBILIZATION
- Includes significant intoxication, dementia, speech or hearing impairment, age (young children), language barrier
- Examples are numbness, focal weakness, focal sensory deficit, parasthesias
- Includes unconsciousness, significant intoxication, dementia, etc.
- Examples are numbness, focal weakness, focal sensory deficit, paresthesias
Contact Medical Control for Additional Orders if Needed